
Back to Articles
Blood Tests Without a Doctor: Doctor vs Direct Labs (2026)
What you can order without a doctor in 2026, how direct labs compare on turnaround and cost, and how to choose the right panel for your goals.
April 28, 2026
1 min read
Vitals Vault Team
Core Essential Wellness Panel
120+ Biomarkers & a thumbprint of your biological age
Includes the depth of physician-backed labs plus AI-reviewed storytelling so you can act on your physiology with confidence.
- 120+ doctor-curated functional medicine tests
- Personalised Action Plan + AI-reviewed clinical summary
- Upload, track, and securely share past reports
- PhenoAge score to measure your biological age
This article explores the evolving landscape of blood testing in 2026, comparing traditional doctor-ordered labs with direct-to-consumer lab options. It explains the differences in access, test depth, cost, and use cases to help readers make informed decisions about when to see a blood test doctor versus ordering labs directly. The post also highlights key biomarkers and practical tips for tracking health trends efficiently.
If you have ever left a doctor’s office with “everything looks normal” and zero next steps, you already understand why direct-to-consumer lab testing has exploded. In 2026, you can often get a high-quality blood panel without a referral, compare results to prior baselines, and act on patterns like insulin resistance (fasting insulin, HOMA-IR), atherogenic risk (apoB, Lp(a)), inflammation (hs-CRP, homocysteine), and hormone status (testosterone, estradiol, thyroid markers) without waiting weeks for an appointment.
The tradeoff is simple: a blood test doctor visit can unlock prescriptions, imaging, and insurance pathways, while direct labs unlock speed, access, and depth. Here’s how to decide, and what you can realistically order in 2026.
What’s different about ordering blood work in 2026?
Three changes matter for patients:
First, the “gatekeeping” model is weaker than it was. Many people can now order labs through direct access platforms that coordinate the required ordering clinician, then complete the draw at national lab networks.
Second, consumers are demanding advanced, prevention-oriented biomarkers that traditional annual physicals often skip, especially apoB, Lp(a), fasting insulin, hs-CRP, ferritin, and comprehensive hormone testing.
Third, “one-off tests” are getting replaced by trend tracking. A single lab value is easy to misread because of hydration, sleep, training load, illness, and lab-to-lab variation. Repeating consistent panels and watching trajectories is often where clarity comes from.
For background on lab quality and standards in the US, most major patient-facing blood testing ultimately runs through CLIA-regulated laboratories (Clinical Laboratory Improvement Amendments), overseen by CMS. You can read more at CMS CLIA.
When does a doctor-ordered blood test still make the most sense?
Direct labs are powerful, but there are still cases where going through a clinician first is the best path.
Do you need diagnosis, prescriptions, or procedures?
A doctor visit matters when blood work is only one step in a larger medical workflow, for example:
- New chest pain, fainting, severe shortness of breath, neurologic symptoms, or signs of infection (you want urgent evaluation, not just labs)
- Symptoms that may require imaging (ultrasound, CT, MRI), endoscopy, biopsy, ECG monitoring
- Conditions that might require medication changes or prescription treatment
Direct labs can inform these conversations, but they do not replace the clinician’s ability to examine you, diagnose, and treat.
Are you trying to route costs through insurance?
If your goal is to minimize out-of-pocket cost through insurance, a doctor-ordered lab can sometimes help, but it is not guaranteed. Coverage depends on medical necessity, your plan, in-network status, and billing policies.
Direct lab routes are often chosen for the opposite reason: predictable pricing and faster access.
Can you order blood tests without a doctor in 2026?
In many cases, yes.
In practical terms, “no doctor referral needed” usually means you do not have to schedule your own physician appointment to request tests. A reputable service can arrange the order appropriately, then you choose a nearby draw location.
This model is especially useful when you are:
- Tracking cardiometabolic risk proactively
- Comparing lifestyle experiments (sleep, training, diet) against objective biomarkers
- Trying to get deeper testing after feeling dismissed or stuck in “watch and wait”
- Building baselines for longevity-focused monitoring
Vitals Vault is designed for that exact use case: 100 to 160+ biomarkers, no waitlist, clinician-reviewed insights included, and draws at 2,000+ Quest/Labcorp locations nationwide, with results commonly available in 24 to 48 hours for many markers.
Explore the full biomarker library at Vitals Vault Biomarkers or go straight to ordering at Checkout.
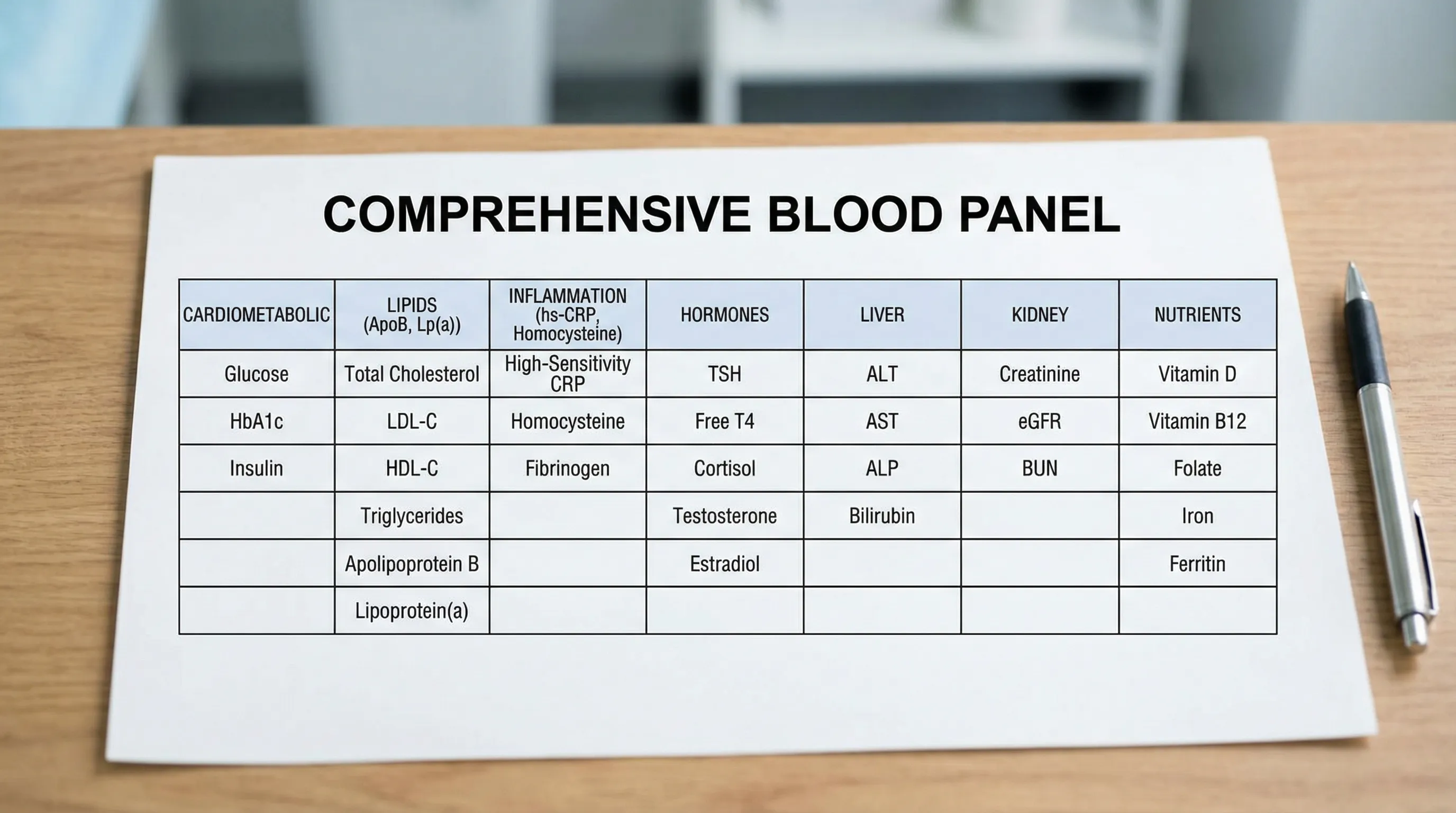
What blood tests can you order directly in 2026?
The short answer: far more than a basic “annual physical panel.” The table below lists high-value categories people commonly order directly for prevention, performance, and longevity tracking.
Swipe
Educational note: which specific tests are available direct varies by state and platform policies, and which are appropriate for you depends on symptoms, history, and medications.
Which tests are “direct-access” friendly, but still require extra interpretation?
Some labs are easy to order and easy to misunderstand. Two examples:
“My LDL is normal. Do I still need apoB?”
Often, yes, if your goal is risk clarity. LDL-C is a cholesterol content measurement, not a particle count proxy in all cases. ApoB can provide a clearer picture of atherogenic particle burden, especially when triglycerides are elevated, insulin resistance is present, or family history is strong.
If you want to go deeper on apoB, Vitals Vault maintains an evidence-led explainer at Apolipoprotein B (ApoB).
“If my hs-CRP is high, does that mean I’m sick?”
Not necessarily. hs-CRP is a sensitive inflammation marker, but it is not specific. Training load, infection, poor sleep, dental issues, and chronic inflammatory conditions can all shift it. It is most useful when you:
- Standardize draw conditions
- Pair it with context markers (CBC, ferritin, fasting insulin)
- Repeat it to confirm trend
Vitals Vault’s deep guide is here: High Sensitivity C-Reactive Protein (hs-CRP).
What can’t you (or shouldn’t you) replace with direct labs?
Direct labs are for measurement, not emergency medicine.
“Should I use direct labs for urgent symptoms?”
No. If you have severe symptoms, rapidly worsening symptoms, or anything that might be life-threatening, seek urgent care or emergency evaluation.
“Can direct labs replace medical imaging or treatment?”
No. Lab data can guide questions, but it does not provide imaging, physical exam findings, prescriptions, or procedures.
“What about abnormal or critical results?”
A high-quality platform should provide clear escalation guidance. You should also have a plan for follow-up, especially for results that are profoundly abnormal, rapidly changing, or paired with concerning symptoms.
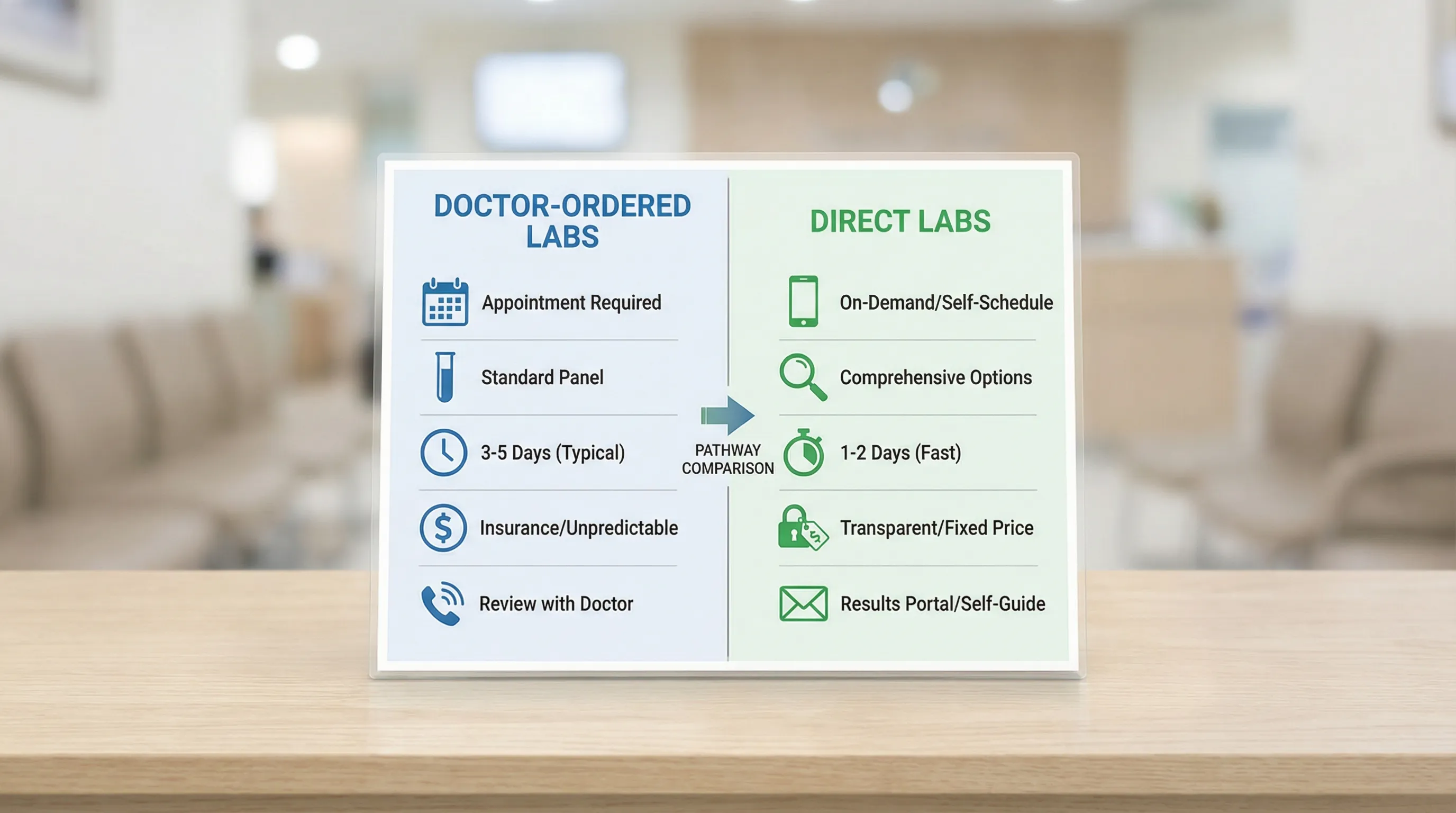
Doctor vs direct labs in 2026: practical differences that matter
Here’s a decision table that reflects how most people actually choose.
Swipe
Vitals Vault vs other direct-lab and longevity testing options (2026)
Not all “direct labs” are equal. Some are marketplaces that sell individual tests with minimal interpretation. Others are longevity programs with clinician review and repeatable panels.
Vitals Vault is positioned as the comprehensive, affordable alternative to Function Health, InsideTracker, Superpower, and Mito Health, emphasizing more biomarkers per dollar, no waitlist, and clinician access included.
Swipe
If you are specifically comparing options, you can also review Vitals Vault’s dedicated breakdowns:
What should you order first if you’re choosing between doctor labs and direct labs?
A simple way to choose is to start with the system you most want clarity on, then add “companion markers” that prevent misinterpretation.
“I feel tired, foggy, or flat. What labs are most useful to start?”
Fatigue is not one biomarker, it’s usually a pattern. Common starting points include:
- CBC plus iron studies (ferritin, iron saturation)
- Thyroid markers (TSH, free T4, and others as appropriate)
- Cardiometabolic (fasting glucose, fasting insulin, HbA1c)
- Inflammation (hs-CRP)
- Nutrients (Vitamin D, B12)
- Hormones when symptoms fit (testosterone, estradiol, cortisol context)
“I want to reduce heart risk aggressively. What should I prioritize?”
The highest-yield add-ons beyond a basic lipid panel are:
- ApoB
- Lp(a)
- hs-CRP
- Fasting insulin and HbA1c (because insulin resistance often drives lipid patterns)
“I’m optimizing body composition and metabolism. What should I track quarterly or biannually?”
People often use a repeatable cadence for:
- Fasting insulin, HOMA-IR (calculated), HbA1c
- ApoB, triglycerides, non-HDL
- Liver markers (ALT, AST, GGT)
- Kidney markers (creatinine, eGFR)
The goal is consistency. Same time of day, similar fasting window, similar training load in the 24 to 48 hours before the draw.
How do you turn direct lab results into a real plan (not just more data)?
The most common failure mode in direct testing is collecting numbers without a decision framework.
“What do I do after I get results?”
A practical workflow looks like this:
- Confirm the draw conditions (fasting, hydration, recent illness, recent intense training, supplements, alcohol)
- Interpret in systems, not single markers (lipids plus inflammation plus insulin resistance, for example)
- Retest to confirm signal when results are borderline or surprising
- Escalate to a clinician promptly when results are clearly abnormal, worsening, or paired with symptoms
Vitals Vault’s model is built around that progression: comprehensive panels, clinician-reviewed insights, and ongoing tracking instead of one-off labs.
If you want to browse specific markers and learn what they mean before you order, start at Vitals Vault Biomarkers. If you are ready to run a comprehensive panel now, go to Checkout.
The bottom line
In 2026, the choice is not “doctor or direct labs.” It is matching the pathway to the job:
Use a doctor when you need diagnosis, treatment, imaging, prescriptions, or insurance-driven care coordination.
Use direct labs when you need speed, deeper biomarker access, and a repeatable system to track trends in apoB, Lp(a), hs-CRP, fasting insulin, HOMA-IR, hormones, liver markers like GGT, and kidney markers like eGFR.
Vitals Vault is purpose-built for the second group: more biomarkers, lower cost, no waitlist, clinician access included, and no doctor referral needed.
Conclusion
Choosing between a blood test doctor and direct labs depends on your needs for diagnosis, treatment, insurance coverage, and speed of access. Direct labs offer greater convenience and biomarker depth for proactive monitoring and trend tracking, while doctor-ordered tests remain essential for urgent or complex medical care. Understanding these differences will help optimize your approach to blood testing and health management in 2026.